
Rachel Bruns continues a series of posts addressing the quality of maternal health care in Iowa. -promoted by Laura Belin
My first post here addressed a number of outdated and non evidence based practices that continue in Iowa. My second post addressed how expanding access to midwives could help improve access to quality care, reduce the incidence of cesareans, and save lives.
This post will continue on those themes addressing additional practices of concern surrounding cesareans and vaginal birth after cesarean (VBAC).
According to the U.S. Centers for Disease Control, Iowa’s cesarean rate is 31.9 percent, meaning nearly one in three births are via c-section. While it is disputed what is a “good” cesarean rate, the World Health Organization states the ideal rate for cesarean sections to be between 10 and 15 percent and that
studies show that when caesarean section rates rise towards 10% across a population, the number of maternal and newborn deaths decreases. When the rate goes above 10%, there is no evidence that mortality rates improve.
I’m not going to focus on the 10 percent of births via cesarean section that are necessary. Instead, I will focus on the surgical births that are preventable, and what may be leading to the overuse of cesareans, which, in and of itself, is jeopardizing lives.
THE ROLE OF HOSPITALS AND PROVIDERS
There is a lot going into that 31.9 percent number. The rate for first time “low-risk” pregnancies is better at 23.7 percent in 2019. The VBAC rate for Iowa is just over 12 percent. Since the VBAC rate is so low (more on that below), we can assume a sizable amount of the cesarean rate is connected to repeat cesareans.
I was part of the one in three Iowa births that happened by c-section. Initially, I thought I fell into the 10 percent of necessary cesareans. My provider used language implying my c-section was inevitable and necessary.
My suspicion based on what I see and hear from other Iowans, in Facebook groups for mothers and other settings, is that many think their c-section was “necessary,” as I did. When a cesarean is necessary, it can be a lifesaving technique, and worth the risks involved, but we can’t all be part of the 10 percent. While I can never prove otherwise, from what I have learned, I now know my cesarean was likely preventable.
So what is causing Iowa’s high cesarean rate while at the same time its maternal mortality rate is increasing? It is well documented that the biggest risk factor for whether someone will have a c-section is the hospital where they will give birth.
I take this a bit further and would say that while the hospital is a factor, ultimately the biggest risk is the provider and their practices. “You can pick a hospital with a low rate, but you don’t know if that individual provider is the one contributing to that,” says Dr. David Lagrew, a maternal-fetal medicine specialist based Orange County, California in this U.S News and World Report article.
Living in Iowa, your options of providers are limited, so the hospital/provider are sometimes one and the same. While the Iowa Department of Public Health has repeatedly rejected my requests for hospital cesarean rates (and my public records request is unanswered to date), there is some hope for improvement. Hospitals will have the option to participate in the Iowa Maternal Quality Care Collaborative’s AIM safety bundle on the reduction of primary cesareans launching later this month.
UNECESSARY INDUCTIONS
One of the more controversial issues facing maternity care is the practice of inducing labor, which is happening for one in four birthing people in the United States. Medical interventions such as inductions can lead to an increased risk of the birth ending in a cesarean. The ARRIVE Study compared induction at 39 weeks to expectant management. Per Evidence Based Birth, the study found,
Inducing labor at 39 weeks did not improve the primary outcome of death or serious complications for babies. For mothers, induction at 39 weeks was linked to a lower rate of Cesarean compared to those assigned to expectant management (19% Cesarean rate versus 22%) and a lower chance of developing pregnancy-induced high blood pressure (9% versus 14%).
Some providers have interpreted this study to suggest they should induce at 39 weeks to reduce cesareans even though the American Congress of Obstetricians and Gynecologists (ACOG) ACOG’s guidelines suggest this is only the case when important factors are considered. If the goal is to prevent cesareans, birthing people would be better off hiring a doula, using a midwife and/or avoiding electronic fetal monitoring as ways to statistically more significantly reduce their risk of a cesarean than a non-medically indicated induction at 39 weeks.
A recent editorial in the American Journal of Obstetrics & Gynecology suggested providers stop calling inductions at 39 weeks “elective” and instead call them “risk reducing.” This is baffling. In 2021, when maternal mortality is increasing, the cesarean rate is too high, and we know what can be done to improve both — they are somehow suggesting that more medical intervention is what is needed and that inductions are “safer” than spontaneous vaginal birth!? Ironically, this same editorial made the point that inductions at 39 weeks for gestational diabetes is based on “weak evidence.” Why then are so many providers in Iowa recommending induction for gestational diabetes at 39 weeks?
As noted by this response to the editorial from the International Cesarean Awareness Network,
If induction was the answer to the high cesarean rate, we wouldn’t have a high cesarean rate anymore […]
There is no standard practice for induction, as methods vary by provider, even within the same clinic. Some wait 10 hours, others wait 40. Some break your water and crank up the Pitocin immediately, others don’t.
If your provider starts calling a scheduled induction at 39 weeks “risk reducing,” then that may be a sign to find a new provider.
While there most certainly is a role for inductions, that intervention is overused. For many an induction will be unsuccessful for a variety of reasons. In my case, I was labeled “failure to progress” based on outdated guidelines. In 2014, the Society for Maternal-Fetal Medicine and ACOG released a consensus statement called “Safe Prevention of the Primary Cesarean Delivery,” stating that Friedman’s Curve should no longer be used as the basis for modern labor management. Per Evidence Based Birth on a study comparing the old Friedman’s Curve and the new guidelines, “Women who received the old model of care (strict adherence to Friedman’s Curve) had a Cesarean rate more than twice as high as the women in the new model of care group: 22.2% vs. 10.3%.”
Many factors play into why a birth may arrest and be labeled “failure to progress, which you can read more about here. Per these updated guidelines, I should not have been induced or labeled failure to progress, and I know that is the case for many birthing people in Iowa, seven years after those updated guidelines were released.
A “TOO BIG” BABY
Hands down the most common issue I hear from other birthing people is that their provider is concerned about them having a “big baby,” which then leads to the suggestion they should schedule a cesarean or be induced to avoid the baby getting “too big” for a vaginal birth. From Evidence Based Birth,
If a care provider thinks that you are going to have a big baby, this thought is sometimes more harmful than the actual big baby itself. This is because the suspicion of a big baby leads many care providers to manage labor in a way that increases the risk of Cesarean and complications.
We know that ultrasounds are not an effective tool to estimate the baby’s weight and they are often off by 20 percent either way. From a New York Times article on the subject of big babies:
“We really urge caution because our tools for identification of a large fetus are so poor,” said Dr. Aaron B. Caughey, “We just aren’t very good at predicting birth weight — every study in the literature would tell you that.”
I can tell countless stories from people that were told they would have a big baby only to go on to have an average 7 pounds baby or the reverse – friends that have given birth to babies weighing more than 11 pounds and their provider was shocked because they had no clue.
In 2016, ACOG released an opinion stating, “induction is not recommended for women who are pregnant with suspected big babies, because induction does not improve outcomes for mothers or babies.” From the American Academy of Pediatrics: “Being born even a week or two early can cause a baby to have trouble breathing, eating, and maintaining a normal and steady body temperature.”
THE BABY’S POSITION
Something I never heard my OB-GYN provider (or hospital based childbirth education course) talk about during prenatal visits was how important the position of the baby was during labor, something I now know to be of the utmost importance. After my cesarean, the OB-GYN who performed the surgery told me the baby was in the occiput posterior position and said she would have been “stuck” so it was a good thing we had the c-section.
While that position does increase challenges with labor, my VBAC baby was positioned the same way. Once my skilled provider (a certified nurse midwife) performed a manual rotation, my son was born vaginally soon after. While there are no guarantees when it comes to birth, birthing people can do a lot of things to improve a baby’s positioning, both as part of their prenatal care and/or during labor including seeing a Webster Certified chiropractor, spinning babies, prenatal physical therapy, and having a doula.
ELECTRONIC FETAL MONITORING
One of the biggest regrets of my VBAC birth is that I succumbed to the pressure of using continuous electronic fetal monitoring (EFM) despite the lack of evidence supporting its use. Per Evidence Based Birth on fetal monitoring:
Randomized trials have found that EFM has contributed to an increase in the Cesarean rate, without making any improvements in cerebral palsy, Apgar scores, cord blood gases, admission to the neonatal intensive care unit, low-oxygen brain damage, or perinatal death (which includes stillbirth and newborn death).
At this point I assume most, if not all, Iowa hospitals “require” electronic fetal monitoring, whether continuous or intermittent. Some may have wireless monitors that allow for freer movement or going in a tub of water, which is ideal. Nevertheless, such policies raise the question: why are hospitals continuing a practice that we know causes more harm than good, compared to the “hands-on listening” approach, which is evidence-based and recommended in practice guidelines? (Note: I know the answer, and if you are interested you can read more here.)
BREECH OR TWIN BIRTHS
Another issue likely impacting cesarean rates is the lack of skilled providers in Iowa who can support breech vaginal delivery and twin vaginal delivery. Canada recently updated its breech guidelines, refocusing them on the importance of informed consent and the training of providers. Breech Without Borders is a nonprofit that provides training to providers on breech birth, since the skill has been lost in most U.S. based obstetrics training programs.
ACOG guidelines support twin vaginal delivery, yet 75 percent of twins are delivered via cesarean in the United States, even though research shows outcomes are improved for twins delivered vaginally. Finally, few providers in the Des Moines area offer external cephalic version for breech presentation as a way to avoid a cesarean, as recommended in ACOG guidelines.
What will Iowa’s obstetric training programs do to improve provider skills in these areas?
C-SECTIONS WITH TUBAL LIGATION
I have heard of some people opting for a repeat cesarean in order to have a tubal ligation performed at the same time. This is logical to avoid a second surgery if a tubal ligation is something you have planned. Unfortunately, some hospitals in Iowa are no longer providing tubal ligations due to teachings of the Catholic Church, with which the hospitals are aligned. Some patients in other states have been successful at suing the hospital for discrimination to force them to perform the tubal ligation.
While I think anyone who wants a tubal ligation should have that option, I also hope people are not opting for a repeat cesarean solely for that reason if a vasectomy, which is safer and more cost-effective, could be a workable option for their family. I recognize vasectomies may not be a viable alternative form of birth control for everyone for a variety of reasons, but it is interesting to look at a close-to-home comparison.
The vasectomy rate in the U.S. is half that of Canada and among American couples, females are sterilized at twice the rate of males. In Canada, vasectomy is twice as common as female sterilization.
Why does this matter? Well for one, tubals are more painful, more invasive, and the recuperation time much longer. And worse, while a failed vasectomy (exceedingly rare) is more likely to end up in a normal pregnancy, a failed tubal ligation can result in an increased risk for ectopic pregnancy, one of the leading causes of maternal mortality.
I do not know if some providers may be suggesting tubal ligation as a benefit of repeat cesareans in lieu of counseling VBAC as an option, but the data is clear they are probably not talking about vasectomy as an alternative. Dr. Esgar Guarín, an Iowa-based family physician and board member of World Vasectomy Day, recently launched a mobile clinic across Iowa to to help increase awareness and access to vasectomies.
VAGINAL BIRTH AFTER CESAREAN
Now on the subject of VBAC (vaginal birth after cesarean). It is no longer the case that “once a cesarean, always a cesarean.” ACOG’s guidelines have continued to support this for more than ten years with several updates. Its most recent policy statement in this area, from 2019, states, “Most women with one previous cesarean delivery with a low-transverse incision are candidates for and should be counseled about and offered” a trial of labor. It also says, “Women with one previous cesarean delivery with a low-transverse incision, who are otherwise appropriate candidates for twin vaginal delivery, are considered candidates” for a trial of labor.
ACOG clarified its stance on Vaginal Birth After Two Prior Cesareans (VBA2C) in December 2016, stating,
Most women with two previous low-transverse cesarean deliveries are candidates for and should be offered TOLAC [trial of labor after cesarean] and counseled based on the combination of individual factors that affect their risk and probability of achieving a successful VBAC.
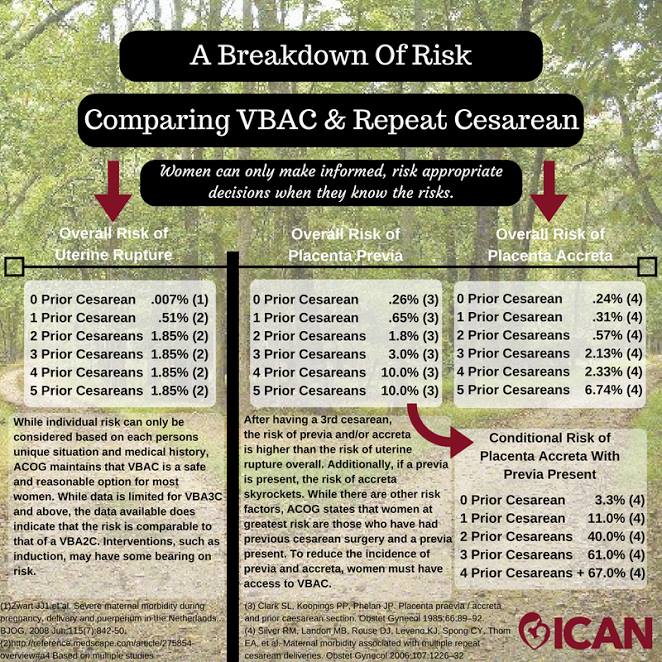
A “trial of labor after cesarean” refers to the labor, not the mode of birth. That practice can result in a vaginal birth or a surgical one. As I have stated before, there is no risk-free birth. You can learn more about the risks of VBAC compared to risks of repeat cesareans here.
{kind=link}
Unfortunately, finding a supportive provider offering VBAC care can be challenging in Iowa, depending on where you live. According to a 2019 study conducted by two certified nurse midwives at the University of Iowa Hospitals and Clinics, 24 hospitals in Iowa offered a trial of labor for one prior cesarean and only ten offered a trial of labor with two prior cesareans. Ten of the hospitals offering that option for one prior cesarean are level I hospitals (the lowest level of care for hospitals in Iowa). Two of the hospitals offering it after two prior cesareans are level I facilities.
While 24 out of about 60 hospitals sounds okay, the reality is that even if your hospital “provides VBAC services,” whether you can find a supportive provider is another question. That became my dilemma in the Des Moines metro, as I learned was true for many others interested in VBAC. According to the International Cesarean Awareness Network, “Forced repeat cesareans due to policy are a violation of patients’ bodily autonomy and the right to informed consent or refusal. We believe these actions are a form of obstetric violence.”
I provided public comment during a July 2018 Broadlawns Board of Trustees meeting (read my remarks and stories from others submitted) taking issue with their policy to “not provide VBAC services” and detailing the challenges of finding a supportive VBAC provider in Des Moines. On principle I believe Broadlawns should offer VBAC services, because as a hospital with a labor and delivery unit they have the capacity to respond to an emergency that may require a cesarean, VBAC or not (i.e., cord prolapse, etc.) as is the case for all 40 level I hospitals in the state.
Note: Broadlawns’ OB-GYNs occasionally take on VBAC patients who have had at least one prior vaginal birth on a case-by-case basis. But they continue to limit VBAC overall and limit access to their certified nurse midwives to care for VBAC patients. I also want to acknowledge they are taking a positive leadership role in training family physicians to work in rural communities, including providing c-section training).
I really don’t want to pick on Broadlawns, because I know based on old data and word of mouth their overall cesarean rate is low compared to other hospitals in the state. In addition, they are not the only ones limiting access to VBAC. What is more outrageous is we have two level III hospitals (same level as the University of Iowa Hospitals and Clinics, the highest level in the state) in Des Moines yet very few providers there truly support VBAC.
I say “truly” because birthing people in our local ICAN chapter will describe “bait and switch” scenarios with several providers who claim to be VBAC supportive, only to start suggesting a repeat cesarean at their 36 week appointment. Alternatively, they may say you “have” to go into spontaneous labor by 39 weeks to have a trial of labor, or you can’t be induced when that may be what is necessary — all things that are out of sync with ACOG guidelines and the evidence on VBAC.
Several providers in the metro are also using harmful VBAC calculators to dissuade or screen out their patients from having access to VBAC care. ICAN has a statement on VBAC calculators here as part of its larger statement on the ACOG VBAC Guidelines. VBAC calculators are racist – with two race-based correction factors, one for “African Americans” and another for “Hispanic” that systematically assign a lower chance of successful VBAC than a white person. Per Evidence Based Birth on VBAC Calculators and Race,
There is a significantly higher likelihood of VBAC among white mothers compared to black, Asian, and Latina mothers. This is not because black, Asian and Latina mothers are physically incapable of having a VBAC. It’s because the system is set up to discriminate against them.
Race is just one problem related to the calculators. They were not meant to be screening tools; rather, they were designed as education tools for birthing people to understand the risks. Instead providers have turned them into inaccurate predictors of VBAC success, usurping patients’ rights to the care they prefer (not undergoing major abdominal surgery). Most people who have a trial of labor will have a successful VBAC (60 percent to 80 percent in hospital settings, depending on the study, and 90 percent in home birth settings).
It is not unusual for birthing people in Des Moines to drive two hours to Iowa City or Omaha, where they are more likely to find supportive VBAC care. I ended up doing this and I continually think of the privilege afforded to me to be able to go that far for both prenatal care and birth. I know that is not an option for everyone, due to challenges with transportation, child care, supportive employer, supportive partner, and so on. Some may be surprised to learn that one of the more VBAC friendly hospitals in Iowa with VBAC supportive providers is in a mid-size community at a level II hospital where certified nurse midwives have been empowered to manage VBACs and they support the practice after two cesareans.
All this tells me individual providers are the hurdle to VBAC access in Iowa, not the safety of VBAC itself.
If Iowa is going to decrease our cesarean rate, we must increase access to VBAC. So many women are being pressured into unnecessary and unwanted repeat cesareans. Many providers are not even telling their patients, especially those who may want big families, about the increased risk of placenta abnormalities like accreta, which are on the rise due to cesareans.
FINAL THOUGHTS
At the end of the day, all I want is for birthing people to be informed so they can make the decision that is best for them and their family, and be supported in that decision. For some that means trying for a VBAC, and for others that means a repeat cesarean. Unfortunately, many people who want a VBAC in Iowa do not have that as a genuine option. Some have to struggle through unsupportive and mentally exhausting prenatal care and birth environments, while continually stating their informed refusal.
It is long past the time for the practice of obstetrics to start practicing informed consent, which means providing their patients with all the information on all the options, not just the one the provider prefers.
I have not even touched on the issue of how providers are paid more for cesareans than vaginal birth, something I normally prefer to avoid discussing, because even with all my frustration regarding maternal healthcare in our state and country, I don’t want to believe cesareans are being performed more for the money. However, it is commonly discussed as one factor in the high cesarean rate. In 2018, California’s state’s health insurance marketplace announced all in-network hospitals must meet a target for low-risk c-sections or risk losing their in-network designation.
The financial pressure is working, along with the implementation of a toolkit led by the California Maternal Quality Care Collaborative that “addresses hospital culture and ways to support vaginal birth, how to manage abnormalities during labor without defaulting to C-sections, and how to use data to push for a reduction in low-risk c-sections,” as detailed in this article by U.S. News and World Report.
I’ll end on this quote from the same U.S. News and World Report article:
The data is there – we know what evidence-based care looks like,” Dawn Thompson, a doula in San Diego says. “But it’s not what’s being practiced, and there’s no motivation for the system to change – there hasn’t been until just recently.”
Nothing in this post should be misconstrued as medical advice or anything other than my personal opinion. Please feel free to reach out to me at rachel.m.bruns@gmail.com.