
Rachel Bruns is a volunteer advocate for quality maternal health care in Iowa.
A 2022 report from March of Dimes shows that “36% of counties nationwide — largely in the Midwest and South — constitute ‘maternity care deserts,’ meaning they have no obstetric hospitals or birth centers and no obstetric providers.” While their report does not provide state rankings, you can see whether your county classifies as being a maternity care desert here. Additionally, a report from Stacker in June 2022 ranked Iowa eleventh on a list of “states where the most people live in maternal health care deserts.”
Even if your area has maternal health care providers (OBGYNs, family physicians, midwives), finding quality care is another challenge facing pregnant and postpartum individuals in both urban and rural areas. I’ve discussed some of those problems in previous articles for this website.
The good news is relatively low-cost, evidence-based solutions are available to make maternal health care more accessible in Iowa, which would improve outcomes. I have identified and prioritized opportunities that should be bipartisan based on successes in other states.
Note: I am not including abortion access in these recommendations, since the procedure continues to be legal in Iowa, the media regularly cover this topic, and several organizations advocate on this issue. This article from Commonwealth Fund explains how states with restrictive abortion laws have worse maternal health outcomes.
The following are five policy solutions legislators and Governor Kim Reynolds can implement as part of the 2023 legislative session to improve maternal health care access for Iowans.
1. Expand Medicaid coverage to 12 months postpartum.
A policy priority that is universally supported by hospitals, providers, and advocates is the need to expand Medicaid through twelve months postpartum. Federal law requires states to provide coverage through 60 days postpartum and the American Rescue Plan in 2021 provided a new provision that allows states to expand coverage to twelve months postpartum to address gaps in care. Just in recent weeks, Congress made this option to states permanent in the FY23 Omnibus.
As of December 2022, 27 states have expanded Medicaid coverage to twelve months postpartum, with seven more planning to adopt. If Iowa implemented this policy, it would have a significant positive impact on Iowans in every legislative district, given that 40 percent of Iowa births are covered by Medicaid.
The Iowa Maternal Mortality Review Committee, which includes a committee of physicians, nurse-midwives, and public health officials in Iowa, recommended expanding Medicaid from 60 days to twelve months postpartum as part of their 2021 report. The same report noted that maternal mortality and morbidity was on the rise across the country and in Iowa. The leading causes of pregnancy related death in Iowa between July 2018 through calendar year 2019 were preeclampsia/Eclampsia, hemorrhage, and suicide. The report concluded that 100 percent of those deaths were preventable.
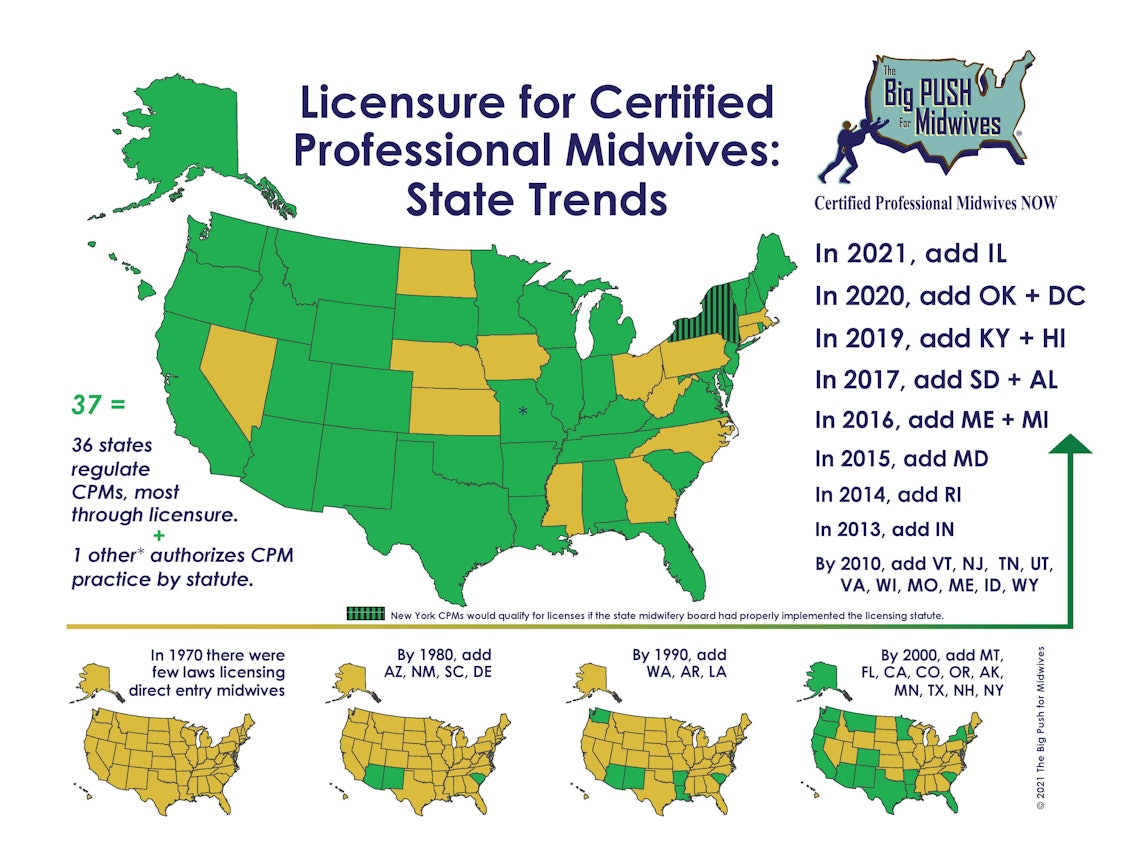
2. License Certified Professional Midwives (CPMs) in Iowa.
Per the World Health Organization, midwives are able to meet the needs of 87 percent of all women and newborns. Research demonstrates that integrating midwives into pregnancy and birth care leads to higher rates of physiologic birth, breastfeeding, and vaginal births after cesarean; decreased rates of obstetrical interventions; and fewer neonatal harms such as preterm birth, low birth weight, and neonatal death.
Despite that evidence and the known obstetrics physician shortage in Iowa, the state of Iowa makes it difficult for Certified Professional Midwives (CPMs) to practice in our state by not offering a license. As of 2021, 37 states and Washington, DC regulate CPMs, including our neighbors in South Dakota, Minnesota, Wisconsin, Illinois, and Missouri.

In 2022, the Iowa House of Representatives passed House File 2547 with tremendous bipartisan support (93 votes to 2) including support from a broad coalition of stakeholders. Learn more about this issue in articles from Iowa Public Radio, Iowa Standard, and Bleeding Heartland. Licensing CPMs would increase access to quality and evidence based maternity care providers.
The only current opposition to this bill is from physician groups and hospitals, which see CPMs as competition. A recent study by Lancet Global Health estimates that even a modest increase in midwife-led care globally could avert a fifth of maternal and neonatal deaths and 14 percent of stillbirths globally by 2035.
If hospitals and physicians truly cared about patient outcomes, they should support this bill, as studies on midwife led home birth indicates integration and licensure of midwives improves outcomes.
I have heard medical providers and lobbyists in Iowa incorrectly refer to Certified Professional Midwives as “lay midwives,” either out of ignorance or intentionally to undermine and condescend. In fact, CPMs have extensive education and training requirements they must meet before practicing. You can read more about the different types of midwives here.
Even the American College of Obstetricians and Gynecologists supports the licensure of CPMs. From the policy statement the organization reaffirmed in 2020:
“The College now also recognizes and accepts the International Confederation of Midwives (ICM)** Global Standards as the common worldwide education, licensure, regulatory and practice standards for midwifery and expresses support for ACNM’s endorsement of the ICM standards. ACOG supports the development of legislation and regulations that utilize the ICM educational standards as the baseline for midwifery education and training here in the United States and the rest of the world. The College supports women having a choice in determining their providers of care. The College specifically supports the provision of care by midwives who are certified by AMCB (or its predecessor organizations) or whose education and licensure meet the ICM Global Standards. The College does not support provision of care by midwives who do not meet these standards.”
The bill the Iowa House approved in 2022 would provide licensure for CPMs that meet ICM Global Standards in alignment with the position of the American College of Obstetricians and Gynecologists. In a forthcoming article, I will write more about the successes and challenges related to this proposed legislation.
3. Provide parity in reimbursement for Certified Nurse Midwives and improve Medicaid reimbursement.
Iowa only reimburses Certified Nurse Midwives (CNMs) at 85 percent of the rate it reimburses physicians when providing the same services for gynecological and obstetrical care such as pap smears, contraceptive family planning, prenatal/postpartum care, and vaginal deliveries. Certified Nurse Midwives should be reimbursed at an equal rate for providing equal services in obstetric and gynecological care.
According to the Iowa Board of Nursing, a CNM is an Advanced Registered Nurse Practitioner, educated in the disciplines of nursing and midwifery who possesses evidence of current advanced level certification by a national professional nursing certifying body approved by the board. The certified nurse-midwife is authorized to manage the care of normal newborns and women for antepartum, intrapartum, postpartum, and gynecologic care.
Iowa has taken important steps to increase access to CNMs through the creation of a CNM education program at the University of Iowa, which is launching this fall. Previously, individuals seeking to become nurse-midwives had to attend a midwifery graduate school in another state. If Iowa wants to be competitive in retaining and attracting a CNM workforce, we need to compete by providing equal pay for equal work.
You can see a comparison of midwifery to physician reimbursement rates by state here. Our neighboring states Minnesota, Wisconsin, Illinois, Missouri, and South Dakota provide 100 percent reimbursement to CNMs compared to physician reimbursement.
In addition to increasing CNM hospital reimbursement to align with physicians providing the same services, we need to increase the reimbursement for Certified Nurse Midwives and OBGYN providers for the global care package, which covers all prenatal, birth, and postpartum care for pregnant and birthing persons. The current reimbursement is so nominal, it is hardly worth the paperwork to become a Medicaid provider. This inordinately affects Certified Nurse Midwives who provide these services for those seeking out of hospital birth.
In fact, these providers are so disincentivized by the nominal Medicaid payment for their services that to my knowledge there is only one home birth CNM practice in Iowa that currently accepts Medicaid. This practice is reimbursed $1,159.80 for the twelve months of care they are providing for each of their home birth clients – including the entire ten months of pregnancy, as well as the two months of postpartum care and any lactation care provided. That is less than $100/month for ensuring the health and safety of an entire pregnancy, vaginal delivery, postpartum course and the health of breastfeeding dyads.
Is that really all the lives of women and infants are worth to us in Iowa? In addition, providers are often not reimbursed by the private insurers that manage Iowa’s Medicaid program in a timely manner. I spoke with one group who has not been reimbursed for any of their births for the entire 2022 fiscal year. With a growing shortage of care providers and settings in Iowa, legislators should be removing financial barriers to providers.
4. Expand access to birth doulas.
The Iowa Department of Public Health noted in its 2021 Maternal Mortality Review Committee report, “structural racism and/or discrimination were determined to be a contributing factor in 40 percent of the cases” of maternal deaths. The same report for 2020 stated, “Iowa’s pregnancy-related maternal mortality was 9.4 per 100,000 livebirths overall…The Black/White ratio is 6.1, Asian/Pacific Islander/White ratio is 3.9 and the Hispanic/White ratio is 1.6.”
In other words, a Black person in Iowa is six times more likely to die from a pregnancy related cause than a white person, and racism or discrimination is a factor in some of these deaths. (Note: While it is important to raise awareness about disparities, I also want to uplift positive stories of birth for Black people. Check out the Birthright podcast for stories of joy and healing in Black birth).
One evidence-based strategy to improve maternal outcomes and reduce disparities is to have a birth doula. According to Evidence Based Birth:
Providing labor support to birthing people is both risk-free and highly effective. Evidence shows that continuous support can decrease the risk of Cesarean, the use of medications for pain relief, and the risk of a low five minute Apgar score. Labor support also increases satisfaction and the chance of a spontaneous vaginal birth. Continuous support may also shorten labor and decrease the use of Pitocin. Although continuous support can also be offered by birth partners, midwives, nurses, or even some physicians, research has shown that with some outcomes, doulas have a stronger effect than other types of support persons. As such, doulas should be viewed by both parents and providers as a valuable, evidence-based member of the birth care team.
Unfortunately, for many people hiring a birth doula can be cost prohibitive. The cost in Iowa can range from $500 to $1,250+ per birth, depending on the doula’s experience level. While some insurance plans will cover all or a portion of the cost of doula care, for most people this is an out-of-pocket expense.
Ideally, the state would require all insurance, including Medicaid, to cover doula care, given its effectiveness at improving birth outcomes and that it saves the state money in the long-run.
During the 2022 legislative session, a group of Democrats introduced Senate File 2013, with the intent to provide doula services to those on Medicaid. Ensuring insurance and appropriate Medicaid reimbursement for doula care would increase access to doulas and improve maternal health outcomes in Iowa. The measure did not advance from a subcommittee, and Senate Republicans voted down a later effort to attach its provisions to a different bill.
You can read more about which states currently reimburse for doula services and more about how doula care is a promising practice to reduce disparities in maternal health via the Doula Medicaid Project. Some positive momentum is that the Iowa Department of Public Health has piloted increasing access to doulas for Black and African American pregnant women through its Title V program.
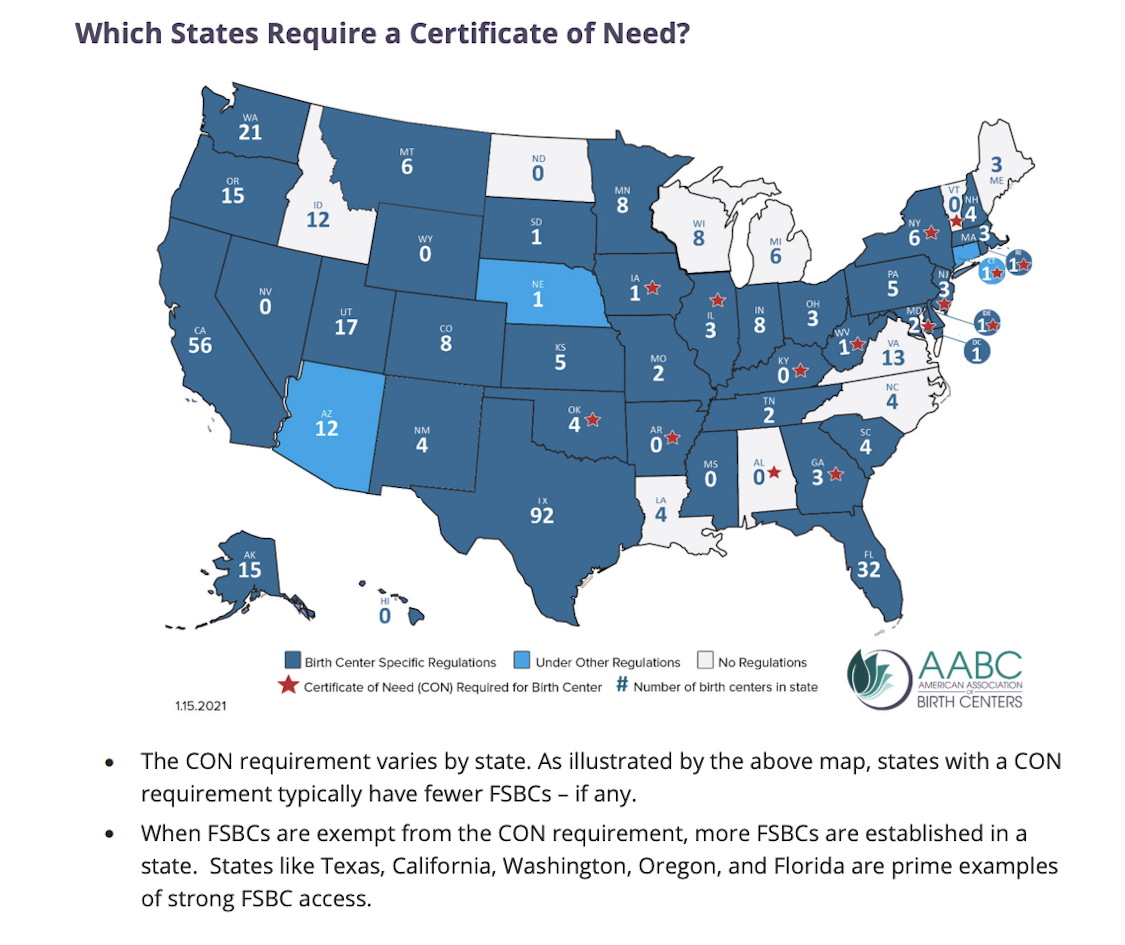
5. Eliminate the Certificate of Need for freestanding birth centers.
As reported by the Business Record, 40 Iowa hospitals have closed their labor and delivery units over the last 20 years. As of April 2021, only 46 counties in the state had at least one open hospital birthing center. At the same time, the state of Iowa continues to make it difficult to open freestanding birth centers. There was one freestanding birth center in the state located in Des Moines; however that birth center recently announced its closure, effective February 2023.
Certified Nurse Midwives have attempted to open birth centers in areas that would benefit from increased access to maternity services. Certificate of Need regulations have kept such birth centers from opening, either directly by local hospitals blocking their opening or indirectly because CNMs cannot afford the costs of going through an expensive regulatory process, especially if it were to be defeated.
According to this position statement from the American Association of Birth Centers, certificate of need laws are associated with fewer birth centers in a state. Research has shown birth centers improve outcomes, narrow racial disparities, enhance patient satisfaction, and reduce costs to state Medicaid programs and other payers. Iowa is in the minority of states that require a certificate of need for birth centers. Among nearby states, Minnesota, South Dakota, Nebraska, Kansas, Missouri, and Wisconsin do not require a certificate of need for birth centers.

Bipartisan bills such as Senate File 2255 (introduced last year) continue to be blocked by the hospital lobby, which is afraid of competition in an environment that desperately needs more quality and affordable options. Removing birth centers from the Certificate of Need process would increase access to freestanding birth centers and improve access to care options.
Numerous studies reaffirm that midwife-led care in community settings (birth center or home) have similar or better outcomes than those who give birth with medical providers in hospitals.
This 2019 report confirmed that birth centers deliver improved health outcomes at a lower cost, averaging 21 percent lower cost of birth and 15 percent lower cost for care for women and infants for the first year after birth.
Another 2013 study found the cesarean rate for women in birth centers is more than four times lower than what is seen among low-risk women in the U.S., creating significant cost savings and reducing preventable cesareans that otherwise could lead to other health problems and challenges with future births.
Of course there is no risk-free birth setting. A 2020 report from the National Academies of Sciences, Engineering, and Medicine stated, “Improving maternity care providers’ and birth centers’ ability to access state licensure and accreditation could also improve access to care.”
The Institute for Medicaid Innovation’s 2020 report on Improving Maternal Health Access, Coverage, and Outcomes in Medicaid indicated that midwife-led care—including in freestanding birth centers—results in improved care, better outcomes, and costs less. From an optimistic perspective I would hope the legislature cares about improving care and outcomes. From a more cynical perspective, I assume they would at least care about saving the state money.
Final thoughts
Iowa is behind other states in implementing proven strategies to improve maternal health.
All of these policies are attainable for Iowa legislators, especially when the state has a large budget surplus. Expanding Medicaid coverage to twelve months postpartum, licensing Certified Professional Midwives, reimbursing Certified Nurse Midwives at the same rate for providing the same services as physicians, providing reimbursement for doulas, and removing barriers to freestanding birth centers are all necessary steps to improve access to care options and outcomes in Iowa.
State policy leaders interested in prioritizing maternal health improvements should review these recommendations from the National Partnership for Women and Families for more information.
I encourage Iowans to contact the Governor’s Office and your legislators to ask them to support these policy priorities in 2023. Additionally, if you are an employer or employee with employee sponsored health insurance (or maybe you work for a health insurance company in Iowa), you can advocate to ensure your plan prioritizes maternal health. Check out this article from BenefitsPro, which highlighted a report from Mercer on six actions employers can take to reduce maternal mortality in the United States.
Feel free to reach out to me at rachel.m.bruns@gmail.com with any questions about these policy ideas. I’m always open to chatting about about maternal health in Iowa.
Top photo of Rachel Bruns provided by the author and published with permission.